
May 4, 2020
Sky-high surprise bills from air ambulance flights possible for many patients
Ground ambulance rides also put majority of patients with private insurance at risk for unexpected out-of-network bills, study finds.

When an emergency dispatcher calls for a helicopter or plane to fly a critically ill patient to a hospital, they don’t have time to check whether they take the patient’s insurance.
Every minute matters for someone badly injured in a car crash, suffering a heart attack or stroke, or needing critical care for serious birth defects, organ transplants or COVID-19.
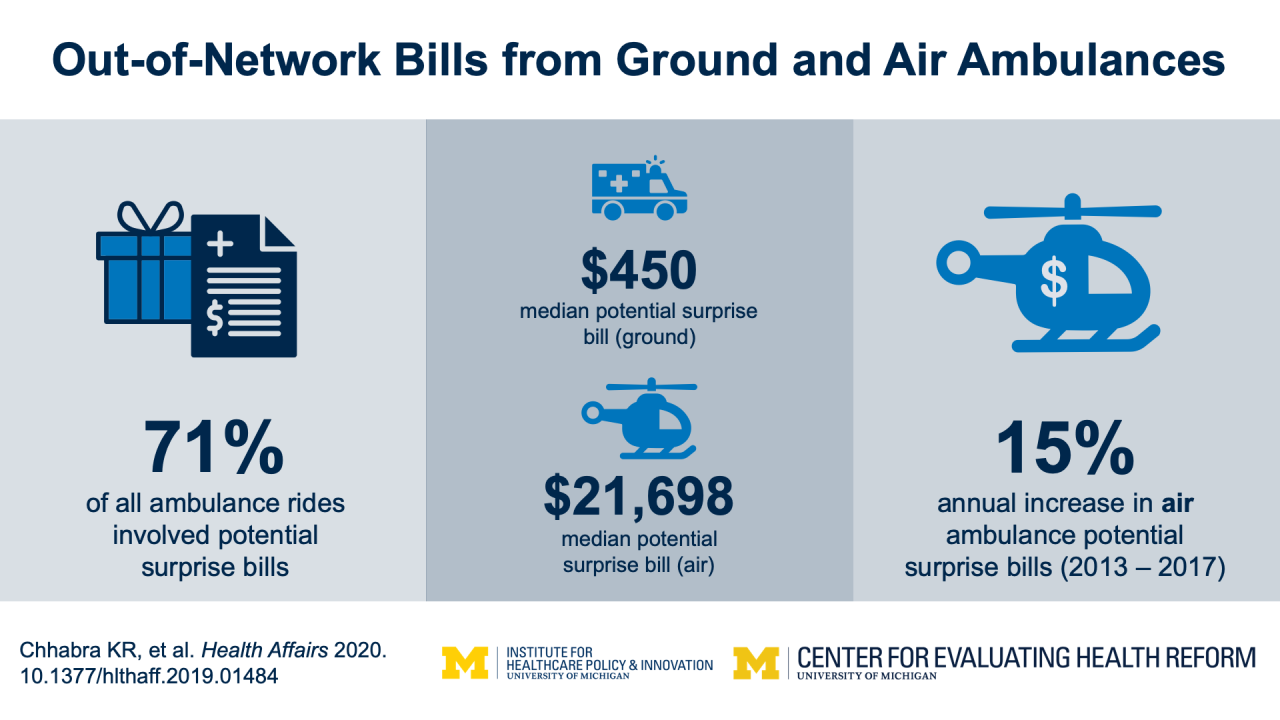
But after those patients land, 72% of them could face a potential “surprise bill” because their ambulance provider isn’t “in network” with their insurance, a new study of people with private insurance finds. When ambulances aren’t in-network, they can charge whatever they see fit, and insurance is not always obligated to pay those charges in full.
So patients could be on the hook for “balance bills” up to $20,000 per ride, the study by a University of Michigan team in the May issue of the journal Health Affairs shows.
Even if the dispatcher chooses a ground ambulance to drive a patient with a medical emergency to a hospital, the study finds that 79% of patients could get a surprise bill, with an average total around $550.
And even for patients who take ambulances for non-emergency reasons, arranged in advance with time enough to check insurance coverage, over half of patients could face a surprise bill for the out-of-network portion of the cost. On average, the study shows that bill could top $400.
The authors note that, while air ambulance charges are high, ground ambulance rides are far more common. As a result, out-of-network ground ambulance bills amount to a larger problem overall: $129 million per year, versus $91 million for out-of-network air ambulances. But annual out-of-network air ambulance bills are catching up quickly.
Shedding light on potential surprises
People with emergency medical needs should never let worries about surprise bills keep them from riding in any ambulance called by a 911 operator, physician or first responder, say the researchers behind the new study.
“Anecdotally, we hear of more people taking Uber or a Lyft, or having someone drive them, to the emergency room to avoid an ambulance bill,” says Karan Chhabra, M.D., M.Sc., a National Clinician Scholar at the U-M Institute for Healthcare Policy and Innovation and surgery resident at Brigham and Women’s Hospital in Boston. “But if you truly need an ambulance, concerns about cost should not get in the way. Arriving by ambulance, with a trained crew that can assess your needs, begin treatment and radio ahead to the hospital, means you’re more likely to be triaged and treated appropriately when you arrive.”
The new study can’t tell how many patients actually got a surprise bill – just how many could have. It’s based on five years’ worth of insurance claims from nearly 1.5 million ambulance transports, including nearly 26,000 by air in the 41 states with more than 50 flights. The study is based on data from patients with commercial insurance offered by one large national company.
Policy implications
Chhabra and his colleagues hope that their work will shine new light on the size and frequency of potential surprise bills from a type of care that federal and state policy fixes often overlook.
Lawmakers have been looking closely at “surprise” out-of-network bills in hospital care, but those occur in only 10 to 20 percent of cases. The new study shows that the risk of out-of-network bills in ambulance-based care is many times higher.
The study also challenges claims by the growing for-profit air ambulance industry that increased competition among service providers would hold down cost growth. From 2013 to 2017, the size of a potential surprise bill for air ambulance rides rose 15 percent, after adjustment for inflation, driven by an increase in the amounts air ambulance companies charged insurance companies for transport of patients.
Air ambulance companies have fought surprise billing legislation in court, using the federal Airline Deregulation Act passed in 1978, which was actually designed to increase competition in commercial airline travel.
Air ambulance companies operating on a for-profit basis have proliferated across the country since the deregulation of the air ambulance industry in 2008. The air ambulance service for U-M’s academic medical center, Michigan Medicine’s Survival Flight, is a nonprofit service that was established in 1984 and does not balance-bill patients.
Future directions
Because of previous research and media reports about surprise bills, policymakers are already assessing potential approaches for reducing the risk to patients. Medicare and Medicaid already bars healthcare providers from sending “balance bills”, to their members.
But patients with commercial insurance — who far outnumber those in Medicare and Medicaid — can still legally be balance billed for out-of-network care in many states. In fact, most patients with commercial insurance cannot be protected by state legislation because their plans can only be regulated federally.
Lawmakers in both chambers of Congress have proposed legislation to end surprise billing, and have even tried to include these fixes in COVID-19 relief packages. Chhabra and the study team believe that protections for patients who require air and ground ambulance care should be incorporated into these federal efforts.
In addition to Chhabra, the study’s authors are senior author Andrew Ryan, Ph.D., a professor at the U-M School of Public Health who directs the Center for Evaluating Health Reform; SPH student Keegan McGuire, resident Kyle Sheetz, M.D. M.Sc., and assistant professor John W. Scott, M.D., M.P.H., of the U-M Department of Surgery, and Ushapoorna Nuliyalu, M.P.H.. Chhabra, Scott and Ryan are members of IHPI, which funded the work.
Study: Health Affairs, DOI: 10.1377/hlthaff.2019.01484


Pay-for-performance and public quality reporting, disparities, healthcare policy analysis

Media Inquiries


