
May 24, 2019
Hospitals fall short in teaching fall prevention to departing patients
rgb(0,46,84)
Falls are a leading cause of hospitalizations and emergency room visits among older adults, but until now, little was known about the relationship between falls and hospital readmissions.

ANN ARBOR—Falls are a leading cause of hospitalizations and emergency room visits among older adults, but until now, little was known about the relationship between falls and hospital readmissions.
A new University of Michigan study found that in people 65 or older, fall-related injuries within a month of hospital discharge ranked as high as the third-leading diagnosis for readmission.
The risk was greater for patients already deemed fall risks, or who were discharged to their homes or home health care.
The findings suggest that by emphasizing personalized fall prevention before discharge, especially for at-risk patients, hospitals could improve patients’ recovery and mobility, and minimize costly fall-related penalties, said principal investigator Geoffrey Hoffman, an assistant professor at the U-M School of Nursing.
The study came about after he and colleagues in a previous study interviewed patients and caregivers about fall prevention, hospital-to-home transition and fall risk awareness. They found that most respondents recalled receiving little fall prevention information at the hospital discharge, though all were considered fall risks.
“Falls are a trifecta in terms of reasons why they need an increased focus,” said Hoffman, who also is a member of the U-M Institute for Healthcare Policy and Innovation. “They are highly prevalent, cause a lot of damage, including death, and they are preventable. However, fall prevention is being left out of the discharge planning conversation and that needs to change.”
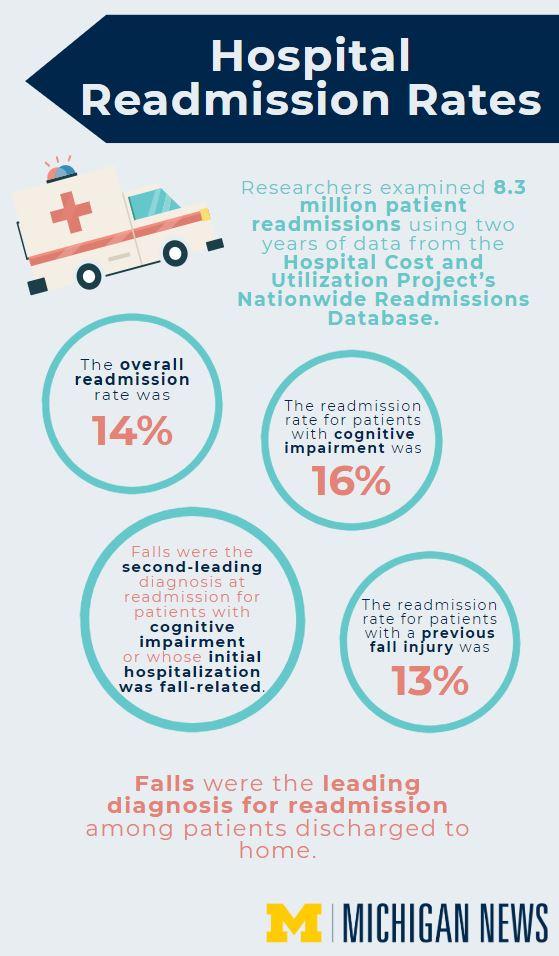
Researchers examined 8.3 million patient readmissions using two years of Hospital Cost and Utilization Project Nationwide Readmissions data. They identified the frequency of fall-related readmissions overall and for two high-risk subgroups: those with cognitive impairment and those whose initial hospitalization was fall-related.
The overall readmission rate was 14 percent. It was a bit higher for those with cognitive impairment (16 percent), but a bit lower for those with a previous fall injury (13 percent).
Falls were the second-leading diagnosis at readmission for patients with cognitive impairment and whose initial hospitalization was fall-related. Falls were the leading reason for readmission among patients whose initial hospital was fall-related and who were discharged to home, even with home health care.
From their earlier interviews, researchers knew that many caregivers and patients perceived the discharged patients’ fall risk as low, even though all were deemed fall risks while hospitalized. Some caregivers were overly cautious, and restricted the patient’s mobility following discharge, which could explain the lower perceived risk.
“After discharge, the goal is to provide patient-centered fall prevention and to safely encourage patients to get up and move,” Hoffman said. “Previous research suggests that in the long-term, limited mobility can harm patients and increase fall risks, something many caregivers and patients may not realize, because sedentary behavior appears to reduce fall risks and falls in the shorter-term.”
Proper education is key, said senior author Lillian Min, U-M associate professor of geriatrics and palliative medicine.
“Discharge planners, doctors, patients and families should develop a personalized plan to balance increased mobility and fall prevention,” she said.
This can include community-based interventions, home modifications and education.
Hoffman said that while the prevalence of fall-related readmissions is high, hospitals can use existing tools to reduce their frequency. Hospitals already know how to identify those with cognitive impairment and fall risk, and have improved their discharge procedures to avoid Medicare’s costly readmission penalty. Now, they just need to include fall prevention in that discharge discussion.
“If they’re in the hospital already, they can be reached with education and prevention before they get home,” Hoffman said.
The study, “Post-Hospital Fall Injuries and 30-Day Readmissions in Adults 65
Years and Older,” will appear May 24 in JAMA Network Open: doi:10.1001/jamanetworkopen.2019.4276

Found in


