
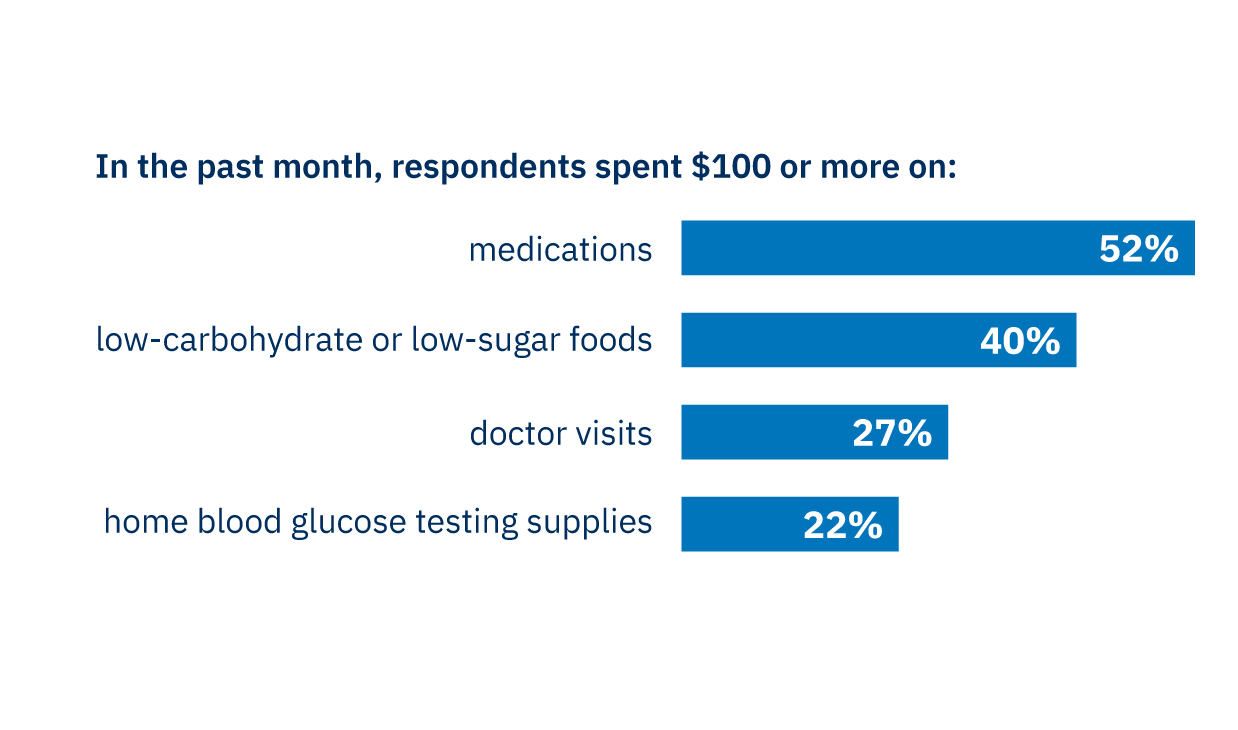
More than half of respondents spent $100 or more out-of-pocket in the past month on diabetes medications. Respondents also incurred significant costs beyond medications.
Key Takeaways
- In a survey of people with diabetes in Michigan, 72% reported high levels of financial stress related to managing their condition, and many experienced substantial out-of-pocket costs. Nearly all respondents were insured.
- Nearly 40% had cut back on healthcare due to cost, including delaying prescriptions or provider visits, or taking less medication than prescribed. This may increase the risk of health complications, hospitalizations, and long-term healthcare costs.
- Policymakers could examine options to reduce healthcare costs for medications and other supplies for people with diabetes, and health systems could screen for cost-related barriers to care, connect patients with resources, and implement financial navigation programs.
Chronic conditions place significant and lasting financial burdens on individuals, even for those with health insurance. Diabetes is a clear example of this challenge and is the costliest chronic disease in the U.S., accounting for nearly 1 in 4 healthcare dollars spent.1 These high costs are driven by both direct medical expenses and indirect costs associated with reduced workplace productivity, lower employment due to disability, and lost productivity resulting from premature mortality. In Michigan, nearly 1 million adults are living with diabetes, costing approximately $13 billion each year due to direct medical expenses and indirect costs.2
Managing diabetes requires ongoing care, which may include taking medications such as insulin, regular blood glucose monitoring, frequent medical visits, and lifestyle modifications such as eating specific foods and maintaining physical activity. As a result, people with diabetes spend more than twice as much out-of-pocket on healthcare as those without the condition.
Over the past decade, states and the federal government have taken incremental steps to address the cost of diabetes care, with a primary focus on insulin. At least 26 states and the District of Columbia have passed legislation to cap monthly copayments for insulin, and some have enacted coverage mandates for diabetes-related supplies and equipment.3 For Michiganders, the most meaningful reductions in insulin costs have come from federal policy changes impacting Medicare: the Inflation Reduction Act of 2022 capped insulin costs at $35 per month for Medicare beneficiaries.
However, emerging evidence suggests insulin cost reforms may not fully address broader affordability challenges. A recent study of nearly 5 million Medicare beneficiaries found that while the insulin cap significantly reduced insulin spending, people with diabetes continued to face substantial out-of-pocket costs for other diabetes-related medications and care.4
The Research
To better understand how financial pressures affect people with diabetes in Michigan, a research team at the University of Michigan surveyed 600 adults with type 1 or type 2 diabetes receiving care at one of Michigan’s largest academic medical centers (data collected in 2019-2021). Nearly all had insurance coverage (98%), either through private insurance (43%), Medicare (30%), Medicaid (13%), or from both Medicare and Medicaid (11%). The researchers assessed cost burden, financial stress, coping behaviors, and health outcomes.
Takeaways from the research
1
Diabetes medications and other expenses related to care and disease management resulted in substantial out-of-pocket costs
2
Financial stress was widespread and linked to worse health outcomes
Overall, 72% of respondents reported high levels of financial stress related to managing their diabetes. Financial stress was higher among those with government-sponsored insurance (64%) compared to privately insured (36%).
Respondents who experienced higher levels of financial stress were more likely to have higher A1C levels, indicating that their diabetes was not under control, greater emotional distress, and more depressive symptoms.
In addition, when reflecting on the impact of their diabetes, many were concerned about their financial well-being:
- 60% worried about financial problems as a result of their diabetes or treatment
- 47% felt frustrated they could not work or contribute as much as usual
- 42% said their medical expenses were higher than expected

3
Many adults cut back on healthcare because of cost
Overall, 39% of respondents reported cutting back on healthcare in one or more ways in the past year because of cost.
Respondents cut back in the following ways:
- delayed filling a prescription (25%)
- delayed seeing a healthcare provider (19%)
- did not fill a prescription (17%)
- took a smaller dose of medication than prescribed (16%)
- skipped a dose of medication (14%)
4
People living with diabetes need help accessing resources — and most are not getting it
When asked where they needed support, respondents most frequently identified needing access to: healthy food (45%), medications and/or insulin (39%), help with medical bills (38%), blood glucose supplies (33%), and other social needs such as housing and utilities (33%). All of the respondents identified at least one need related to managing their diabetes.
Yet most respondents had not accessed available resources to address these needs, with utilization ranging from 4% to 33% across the different resources. In addition, most had never discussed their out-of-pocket costs with a healthcare provider (62%). This highlights a need to connect people with diabetes with resources that can address affordability and reduce financial strain.
What are the implications for policy and healthcare practice in Michigan?
This research finds that Michiganders living with diabetes face persistent out-of-pocket costs for medications, supplies, and medical care that can collectively contribute to significant annual financial burden, even among those with insurance coverage, regardless of whether they were covered by Medicaid, Medicare, or private insurance.. The high costs contribute to cost-related nonadherence, including delayed care and skipped medications, which in the long term could lead to higher downstream spending due to avoidable health complications, emergency department visits, and hospitalizations.
These findings are consistent with national data on diabetes-related financial burden5, suggesting they reflect broader patterns in how insured adults experience the financial demands of managing diabetes. While there have been some changes in policy since these data were collected, the insurance coverage gaps these findings identify remain largely unaddressed for most Michiganders. In addition to cost protections for insulin, policymakers should examine other options to reduce costs for those living with diabetes by requiring that other medications, glucose monitors, and testing strips are covered without cost-sharing.
The findings also highlight a gap in identifying and addressing cost-related barriers in clinical settings as most people reported never discussing costs with their healthcare providers, and few accessed available assistance programs. Healthcare professionals should consider implementing standardized screening for cost-related barriers as part of routine diabetes care, particularly during annual visits, medication changes, or periods of poor glycemic control. Patients who screen positive should be connected to a financial navigator or other resources to address their needs.
Some health systems in Michigan and around the country have developed financial navigation programs for patients with cancer, in which trained navigators help patients identify and access drug assistance programs, food resources, and support for medical bills. These programs are typically funded through a combination of health system operational budgets and philanthropic support, with limited and inconsistent reimbursement through existing care management mechanisms. Health system leaders and health plans should consider extending this model to people with diabetes, where the financial burden of disease management is substantial and the patient population is larger.
Because sustainable funding for this type of support cannot rely on institutional resources alone, policymakers have a role to play. Michigan Medicaid managed care contracts already require health plans to provide care coordination services; incorporating financial navigation into these requirements would be a feasible and concrete extension of that existing framework and could help ensure that high-risk patients receive consistent and equitable support in addressing the financial considerations related to their diabetes care and management.
- Economic Burden, Financial Stress, and Cost-Related Coping Among People with Uncontrolled Diabetes in the U.S. Patel MR, Tolentino DA, Smith A, et al. Prev Med Rep. 2023 May 15;34:102246. doi:10.1016/j.pmedr.2023.102246.
- Financial Toxicity in Diabetes: The State of What We Know. Patel MR. Curr Diab Rep. 2025 May 13;25(1):32. doi:10.1007/s11892-025-01588-0.
- Measurement and Validation of the Comprehensive Score for Financial Toxicity (COST) in a Population With Diabetes. Patel MR, Zhang G, Heisler M, et al. Diabetes Care. 2022 Nov 1;45(11):2535-2543. doi:10.2337/dc22-0494.
- Economic Costs of Diabetes in the U.S. in 2022. Parker ED, Lin J, Mahoney T, et al. Diabetes Care. January 2024;47(1):26-43. doi:10.2337/dci23-0085.
- The Burden of Diabetes in Michigan. American Diabetes Association. Accessed March 19, 2026. https://diabetes.org/sites/default/files/2025-08/michigan-diabetes-08-26-25.pdf.
- Brief: Accessing Diabetes Care and Management. National Conference of State Legislatures. Accessed April 15, 2026. https://www.ncsl.org/health/accessing-diabetes-care-and-management.
- Out-of-Pocket Spending for Insulin by Medicare Beneficiaries After Monthly Caps. Hong D, Cantos K, Morgenstern D, et al. JAMA Intern Med. 2026 Apr 6. doi:10.1001/jamainternmed.2026.0255.
- Burden and Consequences of Financial Hardship From Medical Bills Among Nonelderly Adults With Diabetes Mellitus in the United States. Caraballo C, Valero-Elizondo J, Khera R, et al. Circ Cardiovasc Qual Outcomes. 2020 Feb;13(2):e006139. doi:10.1161/CIRCUITOUTCOMES.119.006139.
Author
For more information, please contact Minal Patel, Professor at the University of Michigan School of Public Health, at [email protected].


