
May 22, 2020
New analysis outlines policy considerations for improving federal Hospital-Acquired Condition Reduction Program
U-M researchers identify potential modifications through rulemaking to federal program focused on reducing complications developed by patients during hospital stays.

Hospital-Acquired Conditions, such as bedsores, infections, and postoperative blood clots, are pervasive and cause unnecessary morbidity and mortality.
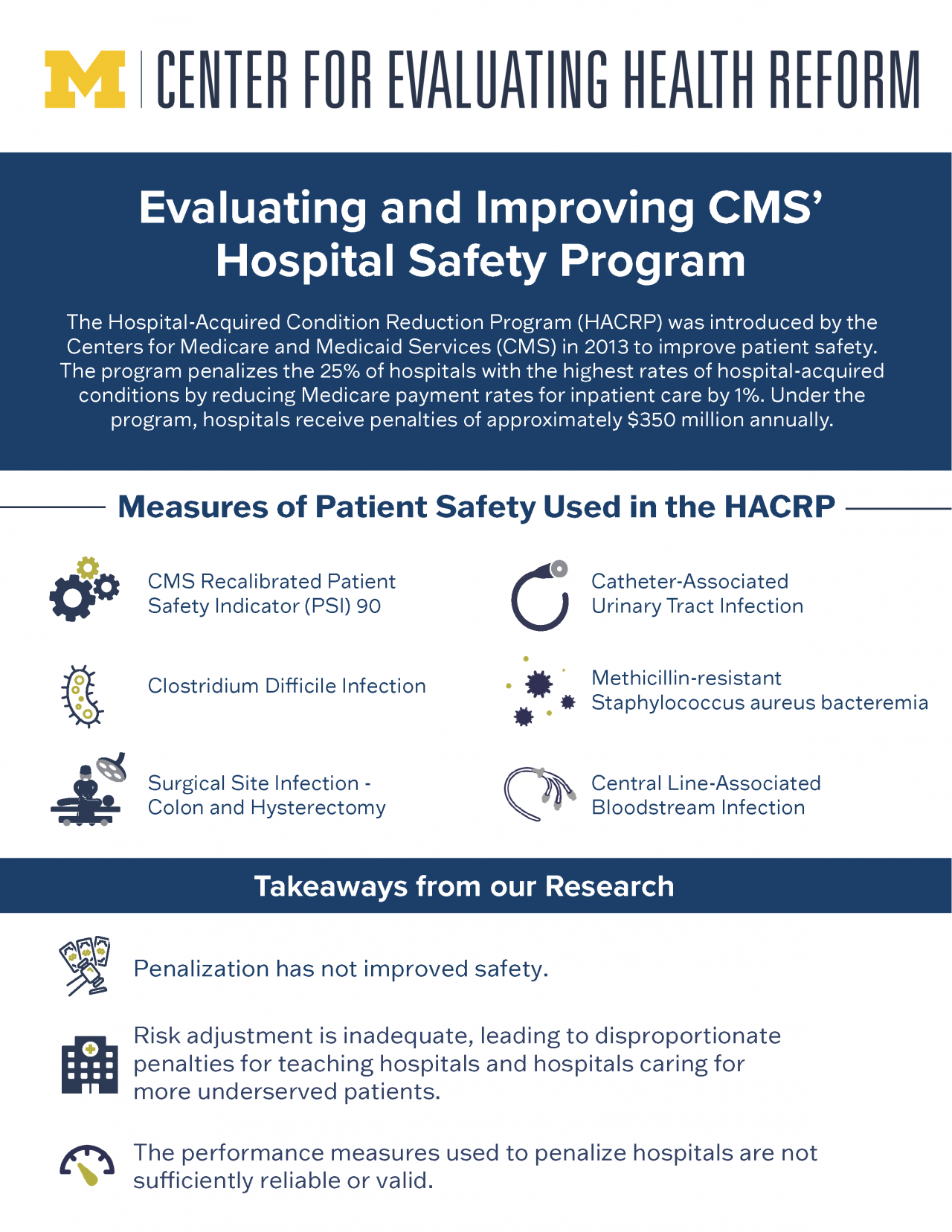
To reduce the rates of Hospital-Acquired Conditions (HACs) and improve patient safety, the Hospital-Acquired Condition Reduction Program (HACRP) was established by the Affordable Care Act in 2013. Under this pay-for-performance program, 25% of hospitals with the highest rates of HACs are penalized with a 1% reduction in Medicare payment rates for inpatient care by the Centers for Medicare and Medicaid Services. Complications that are assessed include the rates of infections, bedsores, sepsis cases, postoperative blood clots, and other preventable hospital-based complications.
Evidence suggests that the HACRP has not driven significant patient safety improvements, according to a new JAMA Health Forum article by a University of Michigan research team.
The authors, Andrew Ryan, Ph.D., M.A, associate professor of health management and policy at the U-M School of Public Health and director of the Center for Evaluating Health Reform, Emily Lawton, a health management and policy Ph.D. candidate, and Kyle Sheetz, a resident surgeon at Michigan Medicine, analyzed the literature on the impact of the HACRP. The evidence indicated that the program has not improved patient outcomes, performance measures used to penalize hospitals may not be sufficiently reliable, and teaching hospitals and hospitals that treat more complex patient populations disproportionately received penalties.
Ryan and the team discuss a series of recommended modifications to HACRP through rulemaking, the process through which the executive branch specifies the details of congressional legislation. The researchers’ recommendations for the Department of Health and Human Services include rewarding hospitals that implement preventative measures, establishing clear guidelines for HAC reporting, and incorporating additional risk factors to improve risk adjustment methodologies. Such modifications to the HACRP may improve the program’s effectiveness, make penalties fairer, and strengthen the reliability and validity of safety measurement.


Pay-for-performance and public quality reporting, disparities, healthcare policy analysis


